
The drug Mifepristone is pictured above. The following article, discussing the use of Mifepristone as an abortifacient, details concerns about that use. No portion of the article constitutes medical advice. D. Joy Riley, M.D., M.A., Executive Director, The Tennessee Center for Bioethics & Culture

Joyce A. Shelton, Ph.D.
Professor of Biology Emerita
Trinity International University
Mifepristone, the so-called abortion pill, continues to be a prominent news topic, particularly since a Senate Committee conducted a hearing in January on its safety, and the landmark Louisiana v. FDA case (enjoined by 10 states), which challenges in-person dispensing requirements, was heard recently in federal court. With the onslaught of information being presented to the public, it is increasingly difficult to evaluate the issues surrounding mifepristone use. What should we know about how this drug works, its safety and efficacy, and how is it being utilized to make chemical abortions widely available without medical oversight?
What is mifepristone and how does it work?
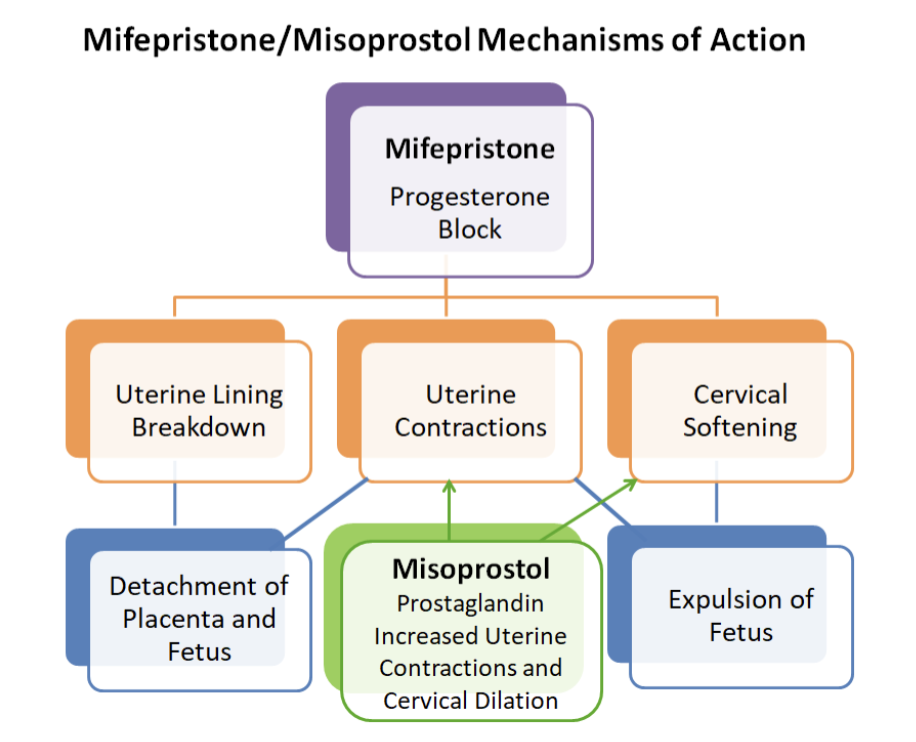
Mifepristone, previously known as RU486, blocks progesterone from binding to its receptors in the uterus. Progesterone is a hormone that is required for the maintenance of pregnancy. The diagram below shows the mechanisms of action for mifepristone and an often accompanying drug, misoprostol, in the inducement of a chemical abortion. (Note: The diagram is not a sequence of events). When progesterone is blocked by mifepristone, the lining of the uterus begins to break down and the placenta along with the growing baby begins to detach. When the blood and nutrient supply is completely cut off, the baby will die. The decreasing progesterone levels also cause the uterus to become more sensitive to prostaglandins that initiate uterine contractions and cause the cervical opening to soften. Eventually the baby is expelled. Abortion providers generally recommend that administration of mifepristone be followed by a second drug, misoprostol. Misoprostol is a prostaglandin, a substance that enhances uterine contraction and helps dilate the cervix. While either drug alone can induce an abortion, one danger is that it will not be complete (the baby/uterine tissues may not be completely expelled). Retaining tissue in her uterus can cause serious harm to the woman and may require surgical removal. Taken together, the two drugs will cause a complete abortion at eight or less weeks of pregnancy about 94-98% of the time and at 10-11 weeks of pregnancy about 87% of the time. The FDA has approved use of these drugs for chemical abortion only up to 10 weeks of pregnancy.
What are the side effects of taking mifepristone?
Even though Planned Parenthood and other such organizations, including the American College of Obstetricians and Gynecologists (ACOG), consistently promote mifepristone, especially in combination with misoprostol, as a very safe method for inducing abortions, the potential side effects and other risks of taking mifepristone are numerous, and some are quite serious. All women who take the drug will experience abdominal cramping, bleeding, and passage of blood clots as consequences of the abortion, but the severity of these effects is highly variable and can be life-threatening. Other serious side effects could include extensive or prolonged hemorrhage, severe abdominal pain, seizure, anaphylactic shock, sepsis, and coma. A complete list of side effects can be found here. In April of 2025, the Ethics and Public Policy Center (EPPC) published an extensive study “based on analysis of data from an all-payer insurance claims database that includes 865,727 prescribed mifepristone abortions from 2017 to 2023.” They concluded that “10.93 percent of women experience sepsis, infection, hemorrhaging, or another serious or life-threatening adverse event within 45 days following a mifepristone abortion.”
Is mifepristone considered safe enough to allow access with little or no medical oversight?
Given the high potential for such serious, potentially life-threatening adverse events, it would seem obvious that mifepristone should be dispensed under medical prescription and supervision to protect a vulnerable or uninformed patient from harm. Indeed, when mifepristone was first approved by the FDA in 2000, there was just such a requirement. The restrictions included at least three in-person doctor visits, prescription by a licensed physician who could determine if the gestational age was within the recommended seven-week period, and follow-up visits to determine that the pregnancy had been terminated and fully evacuated with no adverse effects. However, gradually over time the restrictions on this drug have been modified, reduced, or removed. The biggest change occurred during the COVID pandemic (2020-2021) when clinics were closed, concerns over abortion drug availability were raised, and the ACLU sued the FDA for restricting access. In response, the FDA stated it would not enforce in-person dispensing requirements during the COVID emergency. In 2023, the Biden Administration, with the backing of ACOG and other medical groups, requested further reduction in drug access restrictions. The FDA reviewed “the published literature, other relevant safety and adverse event data and information provided by advocacy groups, individuals, and the applicants related to the modifications that were under consideration.” They then changed the permitted gestational age to ten weeks, removed completely the requirements for in-person dispensing of drugs and allowed prescription online by a “certified provider” who is not necessarily a physician. No in-person or follow-up physician visits are now required. No official reporting of abortions or drug adverse reactions caused by this method is required.
Because of the ease of access, chemical abortions have been steadily on the rise (63% of all abortions in 2025). We might surmise that there would be a concomitant rise in the number of cases of women experiencing serious adverse events. However, because the FDA no longer requires serious adverse events other than death to be reported, such a conclusion cannot be drawn directly. We do know from previous data that chemical abortions have a complication rate of four times that of surgical abortions. The report by the EPPC, despite many partisan detractors, gives clear and convincing evidence that chemical abortions should be cause of community concern for the health and safety of the women being convinced to take these drugs, notwithstanding the children who are being aborted. Women self-medicating with these drugs often bypass the care and advice they could receive from a physician. After all, they have been told that these medications are safe, safer than Tylenol, even safer than having a baby. They don’t always read or follow the lengthy package insert in the pills they receive from an online provider, so they remain unaware of the potential dangers. Many ignore the ten-week restriction on chemical abortions. Often their first encounter with any real medical professional is in the ER. Another concern is that online providers may sell counterfeit or substandard drugs. A newly appearing alarm is that someone else could access the drugs and administer them to the pregnant woman without her knowledge or by coercion. Further complicating the issue is the demise of Roe v Wade and the return of abortion-policy making to the states. Mail-order access has been used to circumvent laws in those states that currently restrict abortions.
Is chemical abortion reversible?
A handful of states now require medical personnel to offer women seeking abortions a chemical abortion reversal option in the form of a progesterone injection within 24 hours after taking mifepristone. Ironically, for many pro-abortion advocates, pro-choice does not mean that women should have the opportunity to change their minds. They have vehemently opposed this option, stating that this drug has not been approved for such a use and, furthermore, most women do not regret their abortions and don’t need such a drug. The American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) supports the reversal option.
Is any current action being taken regarding access to mifepristone?
In April 2025, Senator J. Hawley (R-MO) requested that, in light of the growing crisis with chemical abortions, the FDA review new data about the safety risks of mifepristone use and reinstate previous safeguards as soon as possible. In November 2025, the FDA was requested by 175 House Republicans to investigate the potential safety risks of abortion pills and restore boundaries. A Senate Committee conducted a hearing on January 14, 2026, entitled Protecting Women: Exposing the Dangers of Chemical Abortion Drugs. The Chair, Bill Cassidy (R-LA), and his Republican colleagues emphasized, yet again, the need for the FDA to complete their mifepristone review and take action. The Louisiana v. FDA case, heard in federal court on February 24, 2026, requested that the federal government reinstate restrictions on mail-order prescription of mifepristone. There has not yet been a ruling in this case.
The FDA has acknowledged mifepristone concerns and has claimed they are conducting their own study to re-evaluate the safety of the drug. However, according to Senator Hawley and other congressional leaders who met recently with the FDA, they do not seem to be in any hurry to complete it and refuse to take action until they do, even though they are empowered to make changes without it. Hawley has threatened congressional action. The opposition to restrictions on mifepristone is strong (tennesseecbc.org 2025, publichealth.jhu.edu 2026, plannedparenthoodaction.org, the federalist.com 2026). A number of “experts” who testified at the recent Senate Hearing refused to acknowledge mifepristone’s potential to harm women (eppc.org 2026, the federalist.com 2026) and argued that ready access to abortion is the more critical concern.
Meanwhile, an increasing number of hapless women who have been convinced that a DIY chemical abortion is not only the right thing to do, but their right as a woman, are being seriously injured or even killed by these dangerous drugs. These women are part of our community. They are our sisters. We don’t have to affirm their decision to abort their child to guard them from harm. We do owe them true information, hopeful intervention, and honest compassion, while continuing to support, at the very least, the return to restricted access of mifepristone/misoprostol for use in DIY chemical abortions.