
D. Joy Riley, M.D., M.A.
Executive Director
The National Organ Transplantation Act (NOTA) of 1984 established the not-for-profit Organ Procurement Organizations (OPOs). These facilitate the organ donation process in a variety of ways — from public education to “clinical management of organ donors and assessment of medical suitability.” There are 56 OPOs in the United States. Hospitals are assigned to a specific OPO; there is no choice involved. In recent years, OPOs have come under scrutiny due to various negative reports, including the harrowing experience of one family described below. The revealing testimonies by transplant surgeons and others during a 2024 House hearing are well worth your listening time (click on the second image below).
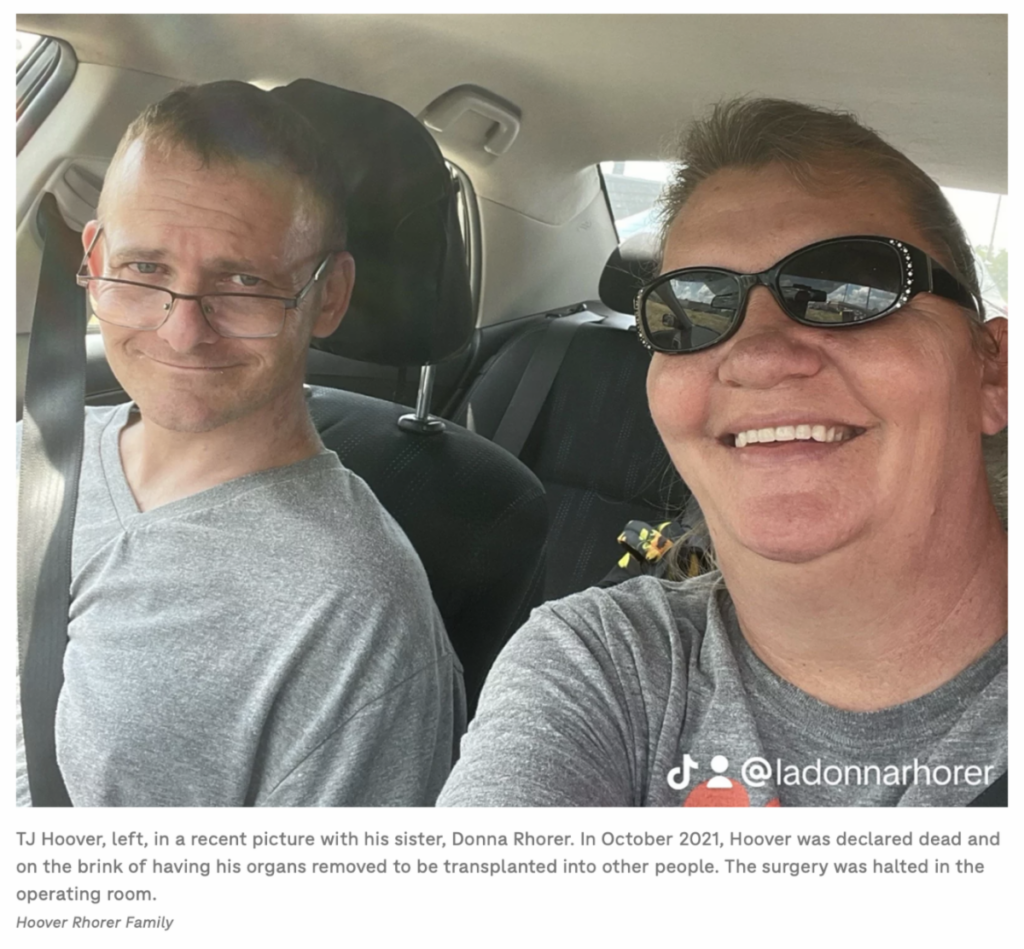
At a Kentucky hospital in October 2021, a man was declared dead, and his organs were to be harvested. In the operating room where the procurement was to take place, he showed signs of life (moving, “thrashing,” crying), and then the planned procedure was aborted. You can read the story here. TJ Hoover is pictured more recently with his sister at left.
Patients and their families are not the only ones worried. In the video linked below, an advocate and several physicians present their concerns as well as recommendations for an overhaul of the Organ Procurement and Transplantation Network (OPTN). Those testifying in the September 2024 U.S. House hearing mentioned allocation out of OPTN sequence, as well as conflicts of interest on the part of principals in the OPTN, among other concerns.

See Dr. Robert Cannon’s testimony at ~28 minutes, followed by that of Dr. Seth Karp (Vanderbilt University Medical Center) by clicking the above link
(16 September 2024 hearing).
This month, the Centers for Medicare & Medicaid Services (CMS) announced some changes . . .
- Medical care comes first: Hospitals must provide complete, life-saving medical treatment without regard to potential organ donation.
- Families are given time to make an informed decision: Families must have appropriate time to process their loss before donation decisions begin.
- No coercion: Patients and families are protected from rushed decision-making and inappropriate pressure.
- OPOs cannot influence critical decisions: OPOs are prohibited from influencing the timing of life support withdrawal or death declarations.
- Medical standards upheld: Death must be declared according to accepted medical standards before organ recovery begins.
This is a step in the right direction, and the Tennessee Center for Bioethics & Culture lauds those who are working to improve the organ donation process. Particularly, these concerns need to be addressed:
1) It is imperative that we treat patients well — whether or not they are organ donors.
2) There should be absolutely no coercion for organ donation.
3) OPOs should not be practicing medicine or influencing medical decisions.
We look forward to the implementation of the long-overdue changes announced by the Centers for Medicare and Medicaid Services.
Furthermore, the Dead Donor Rule — an ethical rule that donors should be dead before their organs are harvested, and the harvesting or retrieval of organs must not cause death — should be observed.